As you prepare for the ABOto ENT Written Qualifying Exam, one of the best ways to get ready for test day is by taking practice questions. Otolaryngology questions allow you to review subject areas and get ready for the question types you will see on the exam. See where you stand as you study with these two free ENT questions from the BoardVitals Otolaryngology Question Bank.
Question 1. Rhinology QID 6957
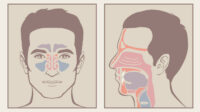
A 24 year-old male presents to you for evaluation of right nasal obstruction and caudal septal deformity. Examination reveals the findings shown. The patient denies any prior nasal surgery. He had nasal trauma as a child from a baseball injury to the nose. The patient is taken to the operating room for an open septorhinoplasty and repair of a large caudal septal deviation. Which of the following techniques is the most appropriate for repair of this patient’s deformity?

A. Extra-corporeal septoplasty.
B. Bilateral spreader grafts.
C. Tongue-in-groove technique.
D. Mustarde-type septal suture.
E. Costal cartilage harvest and placement of large caudal septal extension graft.
Answer: A. Extra-corporeal septoplasty.
Explanation:
A – True – Extra-corporeal septoplasty is designed to repair severe caudal septal deformities such as this one. This technique necessitates that the septum be otherwise largely intact. The entire cartilaginous septum (or the anteriocaudal portion) is removed and a new L-strut carved from the straight cartilaginous portions of the septum after careful measurement of strut dimensions. Given this patient’s severe caudal septal deviation, this procedure would be the most acceptable for this patient.
B – False – Placement of bilateral spreader grafts is quite useful in the correction of dorsal septal deviations but not this type of caudal septal deviation. Spreader grafts are also utilized for repair of internal nasal valve stenosis/collapse.
C – False – The tongue-in-groove technique, as published by Kridel, is useful in repairing mild to moderate caudal septal deviations. In this technique, the caudal septum is sandwiched and sutured to the bilateral medial crura for strengthening and shaping of the caudal septum. A severe deflection such as this one would likely not be amenable to a tongue-in-groove technique only.
D – False – Mustarde-type sutures in conjunction with scoring of the convex side of the caudal septum are useful in the treatment of mild caudal septal deviations. However, as in this patient, suture techniques are not likely to be successful in managing severe caudal deformities.
E – False – Caudal septal extension grafts are often used with extended spreader grafts to lengthen and project the nose. Although a caudal septal graft, such as a septal batten, could possibly successfully treat this caudal septal deformity, there is no indication for costal cartilage harvest in this patient, as he would have sufficient septal cartilage for grafting.
References: 1. Haack J, Papel ID. Caudal Septal Deviation. Otolaryngol Clin N Am 2009 (42): 427-436.
Question 2. Plastic and Reconstructive QID 6886
While you are preparing to perform a right paramedian forehead flap (PMFF) on a 57 year old female to reconstruct her right nasal ala skin defect, you note she has a short forehead. You are concerned about being able to appropriately position the flap. What modification can you perform to increase the flap rotation and improve positioning of the flap?
A. Use a contralateral paramedian forehead flap
B. Create the flap at a more oblique angle
C. Bring the lateral flap incision more inferior than the medial incision
D. Bring the medial flap incision more inferior than the lateral incision
E. Thin the distal half of the flap (remove frontalis and subcutaneous fat)
Answer: D. Bring the medial flap incision more inferior than the lateral incision.
Explanation:
A. While using a contralateral PMFF is acceptable for nasal defect reconstruction, this will result in only a small decrease in the arc of rotation. Consequentially it will have to traverse a farther distance to reconstruct this patient’s alar defect and is a poor choice in a patient with a short forehead.
B. A PMFF is vertically oriented in order to optimize the axial blood flow from the supratrochlear artery. When an oblique skin flap is made this utilizes a more random blood supply to the distal aspect and can result in skin paddle tip necrosis. This will also not change the ability to rotate the flap but would likely increase length of the pedicle.
C. Incorrect, see D.
D. Correct – in order to increase rotation, the medial incision is carried more inferiorly in order to lower and rotate the pivot point. This moves the pivot point closer to the medial canthus and causes the base of the pedicle to be slightly oblique rather than horizontal, resulting in decreased tension when the flap is rotated. Alternatively the flap may be lengthened to reach the defect but this must be weighed against bringing hair bearing skin into the reconstruction.
E. The technique of thinning the frontalis and subcutaneous tissue from the distal aspect is appropriate for a two stage procedure, however this has no effect on the ability to rotate or position the flap. In a two stage procedures the inset with nasal contouring of the distal aspect is performed followed by division of the pedicle with further contouring of the proximal aspect. A three stage procedure includes an intermediate stage for thinning and contouring the distal aspect when the defect is large or includes a cartilage graft. The supratrochlear artery is tightly adherent to the overlying skin at the distal aspect and thus is preserved with this technique.
Reference: Menick F. Nasal reconstruction with a forehead flap. Clin Plast Surg (2009) 36: 443-459.
How did you do? Looking for more ways to review? The BoardVitals Otolaryngology Question Bank contains more than 1,200 questions targeted to the American Board of Otolaryngology (ABOto) Qualifying Exam for Primary Certification, the OTE (in-training exam), and the American Osteopathic Board of Otolaryngology (AOBOO) Written Qualifying Exam. Sign up for a free trial today.