

There has been much cheering about the fact that medical marijuana is now being legalized, but where do we really stand? The answer is that it all depends on where you live and what type of marijuana you want to use. There is no standard state approach to the law. Experts can’t even agree on the number of states that have passed medical marijuana laws. Here are the details.
What is being legalized?
It varies by state. In some states it is medical marijuana, in some it is medical cannabis and in others it is “Low THC, High cannabidiol (CBD) products”.
- Medical marijuana: Whole, unprocessed marijuana used for medical treatments.
- Medical cannabis: Another name for medical marijuana.
- CBD: A compound found in marijuana that has significant medical benefits, but does not make people feel “stoned”. It is one of at least 113 active cannabinoids identified in cannabis.
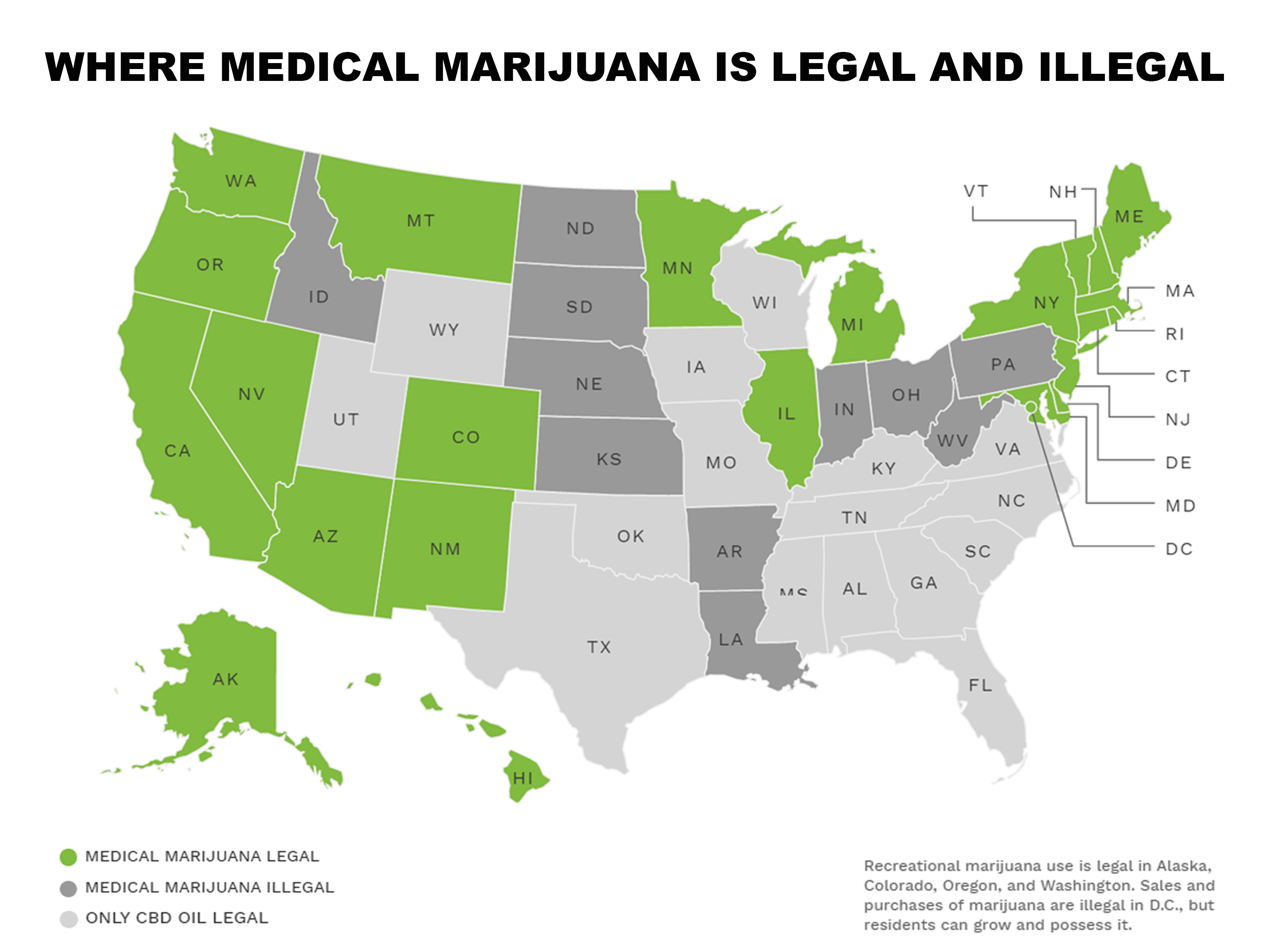
29 states, Washington, DC, Guam, and Puerto Rico have legalized comprehensive public medical marijuana and cannabis programs.
The word “comprehensive” carries legal import in this context. According to the National Conference of State Legislatures, those public medical marijuana and cannabis programs labeled as “comprehensive” carry the following protections for individuals:
- Protection from criminal penalties for using marijuana for a medical purpose;
- Access to marijuana through home cultivation, dispensaries or some other system that is likely to be implemented;
- It allows a variety of strains, including those more than “low THC;” and
- It allows either smoking or vaporization of some kind of marijuana products, plant material or extract.
Separate from these 29 states are 17 states that have passed limited access marijuana product laws. These states allow use of CBD products for medical reasons in limited situations or as a legal defense. In other words, CBD programs are not considered “comprehensive” and do not offer the protections listed above.
What can medical marijuana be used for?
It all depends. (A familiar refrain.) The Institute of Medicine issued a report saying “Scientific data indicate the potential therapeutic value of cannabinoid drugs, primarily THC, for pain relief, control of nausea and vomiting, and appetite stimulation; smoked marijuana, however, is a crude THC delivery system that also delivers harmful substances. The psychological effects of cannabinoids, such as anxiety reduction, sedation, and euphoria can influence their potential therapeutic value. Those effects are potentially undesirable for certain patients and situations and beneficial for others. In addition, psychological effects can complicate the interpretation of other aspects of the drug’s effect.”
The National Academies of Sciences, Engineering, and Medicine released a report that issued 100 conclusions related to effective medicinal uses of medical marijuana and ranked them. Among the findings are:
1. There is conclusive or substantial evidence that cannabis or cannabinoids are effective:
-
- For the treatment for chronic pain in adults.
- Antiemetics in the treatment of chemotherapy-induced nausea and vomiting (oral cannabinoids). For improving patient-reported multiple sclerosis spasticity symptoms.
2. There is moderate evidence that cannabis or cannabinoids are effective for:
-
- Improving short-term sleep outcomes in individuals with sleep disturbance associated with obstructive sleep apnea syndrome, fibromyalgia, chronic pain, and multiple sclerosis (cannabinoids, primarily nabiximols).
3. There is limited evidence that cannabis or cannabinoids are effective for:
-
- Increasing appetite and decreasing weight loss associated with HIV/AIDS (cannabis and oral cannabinoids).
- Improving clinician-measured multiple sclerosis spasticity symptoms (oral cannabinoids).
- Improving symptoms of Tourette syndrome (THC capsules).
- Improving anxiety symptoms, as assessed by a public speaking test, in individuals with social anxiety disorders (cannabidiol).
- Improving symptoms of posttraumatic stress disorder.
A spider’s web of fine marijuana lines by state.
There are many other complications and they change when you cross state lines. Some states require/allow the following while others do not:
- Physicians must write a prescription for medical marijuana. (This requirement is illegal under federal law because physicians cannot prescribe substances listed as illegal by the federal government.)
- Home cultivation of marijuana. At last count 16 of the 28 (or 29) states allow this.
- “Affirmative defense” laws in which arrested marijuana users are allowed to mention medical use in their defense. It prevents conviction but not arrest. (Unless you live in Delaware where the defense is only available between when a patient submits a valid application and receives their ID card, or Ohio, where the defense is only available until 60 days after the state begins accepting patients’ applications.)
- Patient ID cards.
- Patients are registered in a state registry.
All states require proof of residency to apply to be qualifying patients.
If you want an example of how confused legislators are and how convoluted state law can be, just read about the current state of medical marijuana laws in the state of Louisiana, as reported by Karen O’Keefe, JD, Director of State Policies for Marijuana Policy Project (MPP) to the ProCon.org organization:
“In Louisiana, SB 271 was introduced in 2016 to amend a 2015 law that failed to legalize medical marijuana because it said that doctors could “prescribe” medical marijuana, which is illegal under federal law. The new bill changed the wording to “recommend,” which is legal, but did not contain any protections from prosecution for patients, growers, or distributors.
SB 180 was created to close that loophole, but only offered protections for patients who lawfully possess medical marijuana; as a result, the bills did not legalize distribution or cultivation, meaning patients cannot get legal access to marijuana.
In addition, draft regulations would require doctors in Louisiana to list dosage amounts with their recommendations, which may put physicians at risk of violating federal drug laws. For these reasons and others, neither the Marijuana Policy Project nor the National Council of State Legislatures has classified Louisiana as a state with a legal medical marijuana program. This may change depending on how the situation develops in the state.”
Oh and there is one more complication – state vs. federal laws.
According to the NCSL, “At the federal level, marijuana remains classified as a Schedule I substance under the Controlled Substances Act, where Schedule I substances are considered to have a high potential for dependency and no accepted medical use, making distribution of marijuana a federal offense.”
States continue to pass laws legalizing medical marijuana, some of which are null and void because their conditions conflict with federal law. Other states have passed and repealed medical marijuana laws. It’s too convoluted to report here, but suffice it to say that the US Justice Department has reserved the right to challenge the states at any time they feel it’s necessary. That does not provide support and comfort for those looking to expand legalized medical marijuana.
That brings us full circle to our original assessment. What is the current status of medical marijuana laws in the US? It all depends.
If you are a physician who wants to “recommend” (which prescribing is now called to avoid conflict with federal law) medical marijuana to a patient, you should first review the matrix listed on the NCSL site and know the details for your state. The whole thing could go up in smoke before you have the chance to recommend your first non-prescription.
State by State Medical Marijuana CME Requirements
To become a physician who can recommend medical marijuana as a treatment plan to patients, you’ll need to earn CME credits if your state requires it. Because of the novelty of the space, these courses can be hard to find. Each state has different requirements for how many hours you’ll need to complete. Here are the state requirements broken down by state:
Alaska: No CME requirements yet.
- No CME requirements yet.
- The AZ Dept. of Health Services provides a free online CME course regarding the physician’s role and expectations under the AZ Medical Marijuana program.
California: No CME requirements yet.
Colorado: No CME requirements yet.
Connecticut: No CME requirements yet.
Delaware: No CME requirements yet.
Hawaii: No CME requirements yet.
Illinois: No CME requirements yet.
Maine: No CME requirements yet.
Maryland: No CME requirements yet.
- Doctors must complete 2.0 Category 1 CME credits on medical marijuana to recommend
Michigan: No CME requirements yet.
- No CME requirements yet.
- The Minnesota Department of Health offers 22 Medical Marijuana CME credits
Montana: No CME requirements yet.
- 2.0 Category 1 CME credits on medical marijuana to recommend
New Hampshire: No CME requirements yet.
New Jersey: No CME requirements yet.
- 5.0 Category 1 CME credits every 3 years
- Doctors must complete 4.0 Category 1 CME credits to recommend
- Pharmacists must complete 4.0 Category 1 CME credits to sell
- Cost: ~$250
- 3.0 Category 1 CME credits on medical marijuana to recommend
- 1.0 Category 1 CME credit on medical marijuana every 2 years
Vermont: No CME requirements yet.
Washington: No CME requirements yet.
District of Columbia:
- No CME requirements yet.
- The Dept. of Health provides online CE courses on Medical Cannabis.
Deciding Which CME Course is Right for You? Use the CME activity finder tool below to find the online course that best fits your needs and will help you meet your CME requirements. BoardVitals offers online CME activities to make it easy for you to fulfill your requirements, as well as our Pro Plus plan that bundles a gift card with your CME credits.



