If you think that your responsibility as a physician is simply to encourage women to have mammograms, read up- things have changed. Given the recent discrepancies and contradictory recommendations regarding mammography, your responsibility now is to give women the pros and cons of the screening, and make sure they have the information necessary to make an informed choice.
A broad cross-section of research shows that one of the biggest barriers to mammograms is physician-patient communication. When women of different cultures are asked why they do not have mammograms, communication consistently ranks as one of the major reasons.
Appalachian Kentucky Women
(Lower frequency screening, higher mortality rate): When researchers investigated sociocultural barriers to mammography adherence in this population, women described how
“Pain and embarrassment, less personal and less professional mammography experiences, cancer fears, and poor provider communication pose barriers to timely and appropriate mammography schedule adherence and follow-up care.”
African American Women
Mammography screening rates remain lower with African American women than for Caucasian women and breast cancer is a leading cause of death for this population. Researchers explored the reasons for nonadherence to American Cancer Society screening guidelines. Findings revealed that 36% of participants had never received a mammogram, 43% did not have their breasts examined by their doctor once a year, 55% did not perform monthly self-examination, and 23% did not know how to examine their breasts for breast cancer. The most frequently reported reason for not getting a mammogram was because the participant’s doctor had not suggested it.
Immigrant Women
When researchers explored immigrant women’s awareness of, and reactions to, the well-publicized contradictory recommendations on mammography, they found that at least for some immigrant women, “patient-clinician discussions of mammography’s risks and benefits remain infrequent.” The study found that,
“Although immigrant women in our sample were engaged with, and interested in, learning more about mammography and breast cancer, many felt unsure about where and how to seek such information.”

Removing Barriers to Communication
Studies have shown that culture and language are significant barriers to educating women about the pros and cons of mammography in order to create informed decisions. Researchers are finding ways to break down those barriers, as highlighted in several recent studies:
1: A study conducted with Chinese-American women sought to determine how to communicate information about mammography to Asian American women, a population that has experienced a significant increase in breast cancer incidence over the past decade.
Researchers believe that the disparity in late-stage diagnosis and poor survival rates is “due to the utilization rate of mammography and barriers created by acculturation factors such as language, misconceptions and lack of knowledge.”
Personalized messaging seemed to do the trick. When study participants received phone calls with messaging created specifically for them, communication and understanding improved. Eighty-six percent of participants said they received new information about mammography screening that they were not aware of before.
One participant noted: “What you have done corrects the misconceptions that I previously had and gives me correct and updated information about mammograms so I won’t continue to distribute the incorrect information to other friends/women.”
2: A study conducted with Latina women, published in the Journal of Behavioral Medicine found that “Cultural beliefs about breast cancer may act as a barrier to Latina women seeking preventive services or timely follow-up for breast symptoms regardless of access.”
The belief most commonly held was, “Faith in God can protect you from breast cancer” (48 %).
For patients and physicians alike, there is never enough time.
If you could get inside the head of physicians and patients to hear what they think about breast cancer conversations, what do you think you would hear? A study published in the Archive of AMIA Annual Symposium Proceedings gives some insight to that. The study was designed to identify barriers to patient-provider communication when discussing breast cancer risk, in order to aid in the development of decision support tools.
Based on the focus groups held for the study, time constraints, lack of knowledge, low health literacy, and language barriers emerged as the main barriers to communicating risk. The results showed that time was considered as the most significant barrier for both patient and provider groups.
Patients think:
- Providers don’t have much time to explain and the office visit is very hurried so I can’t discuss personal circumstances. I usually have “ten thousand questions.”
- Because we don’t have the knowledge and don’t ask the right questions, the doctor won’t give information to you.
- I want more places to ask questions about breast cancer, even if that person might not be my doctor. It might be a site, a nurse.”
- “I wouldn’t blindly follow a doctor’s recommendations if it’s a general recommendation. I want it to be individualized.”
Providers think:
- I have limited time with patients and when they ask questions toward the end of the visit, it increases time pressure.
- Patients do not know much about medical terms and risk-related numbers, which makes it difficult to communicate risk. The struggle is how to get this information across without creating more anxiety.
- Providers seem frustrated when patients value the doctor’s opinions less and think they know what should be done.
- Providers experienced difficulty when explaining risk to patients mainly due to language and cultural barriers.
How do we achieve informed consent?
There are four important principles that can help you to facilitate informed consent with your patients. You can read the details in the Journal of Women’s Health but the basics are:
- Screening may help, hurt, or have no effect.
- Measuring the efficacy of a screening intervention for one disease is inherently biased due to the nature of data collection and analysis.
- Some screening statistics must be interpreted with caution.
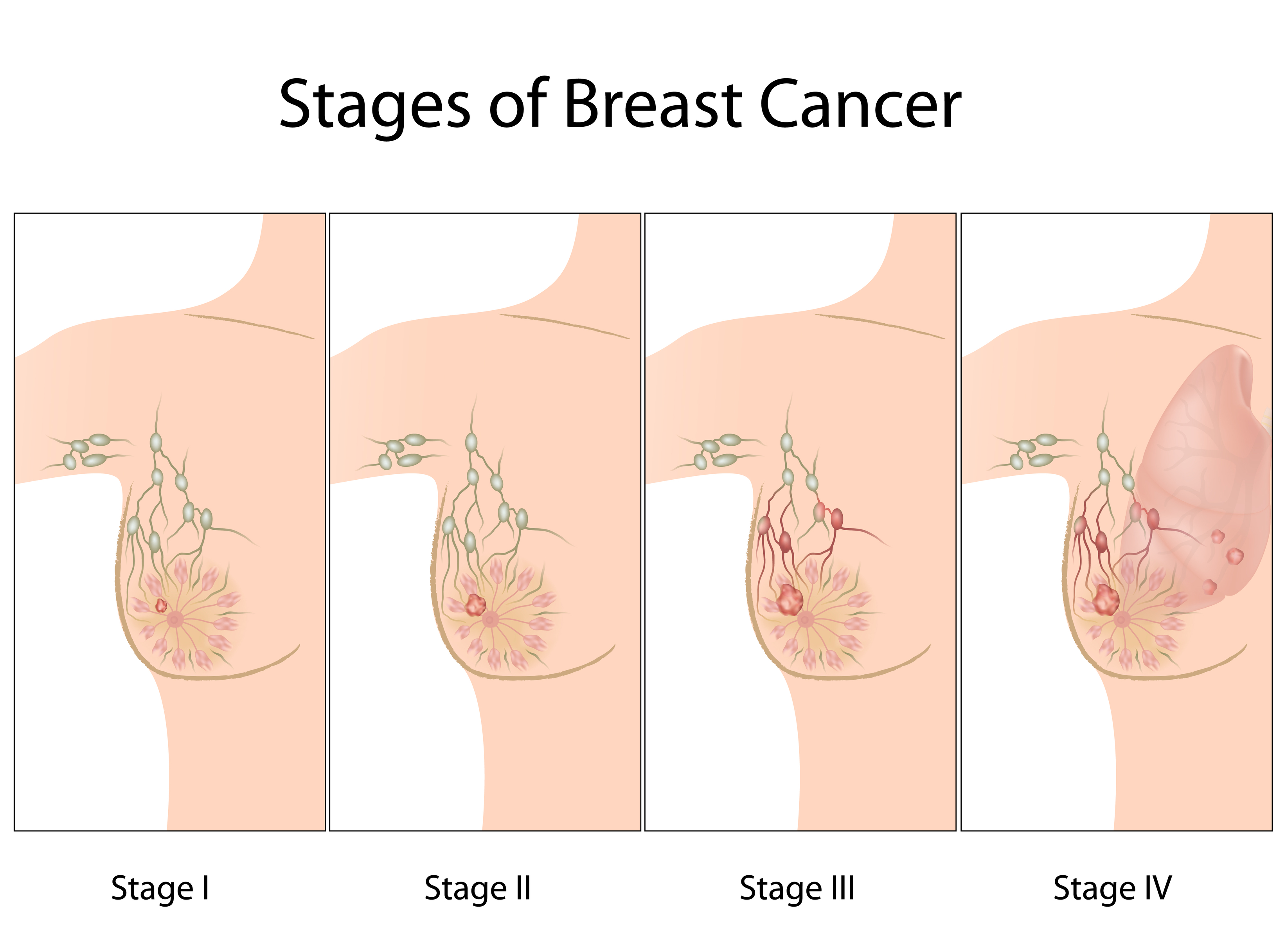
- Since “early detection” is actually late in a tumor’s lifetime, the time window when screen detection might extend a woman’s life is narrow, as many tumors that can form metastases will already have done so.
It’s frustrating that complex, potentially dire medical conditions must be communicated at an elementary level. However, successfully traversing the bridge between a physician’s extensive knowledge and patient understanding is essential if patients are going to truly become engaged in their own care. You may have to discuss the pros and cons of mammography in simple sentences; but when your patient feels well informed and makes appropriate decisions about her care, you’ll be glad you went the extra mile to achieve understanding.