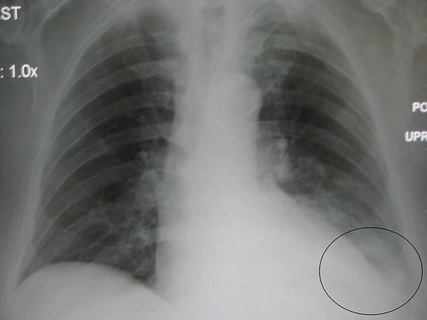
A 45-year-old female with no significant past medical problems presents to your office with a 4-day history of fever and a cough productive of yellow-green sputum. She has had a runny nose, a sore throat, and a dry cough for 2 weeks, which seemed to get better for a couple of days before progressing with her current symptoms. Physical exam is significant for a temperature of 102⁰F and a respiratory rate of 22 breaths per minute. A chest x-ray is shown below. Chest auscultation would most likely yield crackles in which of the following areas?
A. Right Lower Lobe
B. Right Upper Lobe
C. Left Upper Lobe
D. Left Lower Lobe
Answer: D. Left Lower Lobe
Explanation:
The clinical vignette describes a healthy female patient with a recent episode of an upper respiratory infection (URI). Viruses are the most common cause of URIs. However, the scenario in which a URI improves briefly before it develops into a more serious respiratory disease should raise the possibility of a superimposed bacterial infection. This is consistent with the vignette in the question. Bacterial pneumonia may follow a viral URI and present with colored sputum and fever, as described in this vignette. This is further supported by the opacification circled in the image, indicating lung infiltration (for instance, due to infection). In order to standardize localization in chest imaging, the convention is that the clinician is always looking at the image with the patient facing them. Therefore, the patient’s left side is the clinician’s right side, and vice versa. By that convention, the opacified region in the image refers to patient’s the left lower lobe, which is adjacent to the heart (another hint as to the location of the pneumonia). Chest auscultation may reveal crackles over regions of lung infiltration, indicating an abnormal finding (pneumonia in this case). (A) (B) (C) These are wrong since they refer to other lung regions that are clear of any opacities in this image, as they appear as dark areas. Hence, crackles are less likely to be heard over them.
Reference: UpToDate: Diagnostic approach to community-acquired pneumonia in adults Image Reference: By James Heilman, MD (Own work), via Wikimedia Commons
A 3-year-old male patient is brought to the clinic by his mother who states that he’s had this rash for the past few days. She noticed some brownish-yellow crusting on top of the rash. The patient is up-to-date on his vaccines. The mother denies noticing the patient having any fevers, and states that his level of activity has remained the same. On physical exam, his vitals are within normal limits and he doesn’t have any lymphadenopathy. Which of the following is the most likely diagnosis?
A. Strawberry hemangioma
B. Impetigo
C. Erysipelas
D. Herpes Simplex Virus-1 Infection
Correct: B Impetigo
Explanation:
Impetigo is a superficial skin infection that is common in children. It is usually caused by Staphylococcus aureus or, to a lesser extent, Streptococcus pyogenes (Group A strep). The common presentation is a red base with honey-colored crusting. Impetigo commences as vesicles and progresses to a red base with crusting. Topical mupirocin is sufficient for treating small lesions as this one. If multiple lesions are present, oral antibiotics, such as cephalexin and dicloxacillin, are used instead. Notably, it is a contagious condition. Therefore, it is important to implement handwashing among other measures to prevent spreading.
(A) Strawberry Hemangiomas are also known as capillary hemangiomas. They usually appear within days or months after birth, and are the most common benign vascular tumors in infancy. While hemangiomas grow within the first year, they tend to shrink over the next several years. Topical beta-blockers, such as timolol, can be used to help expedite its resolution. Other options include steroids and laser surgery.
(C) Erysipelas is a painful, erythematous skin infection that extends to involve the skin lymphatic vessels. It classically presents with well-demarcated borders, making it relatively easy to diagnose. Group A Beta-Hemolytic Streptoccoci are the main culprit. Erysipelas usually happens in immunocompromised individuals or patients with lymphatic obstruction. Treatment with penicillin is usually sufficient.
(D) Herpes Simplex Virus-1 (HSV1) infection, unlike impetigo and erysipelas, is caused by a virus. HSV1 virus is usually the cause of herpes labialis. In the pediatric population, gingivostomatitis is the common presentation of HSV1. Initially, fever and pharyngeal vesicles appear, with subsequent spreading to the oral mucosa. Cervical lymphadenopathy can be seen. Most infections resolve within a couple of weeks. The patient in the clinical vignette did not have fever or lymphadenopathy, and his rash is not consistent with HSV-1.
Reference: UpToDate: Impetigo ; AskMayoExpert: Infantile hemangioma; UpToDate: Clinical manifestations and diagnosis of herpes simplex virus type 1 infection; Image Reference: By CNX OpenStax CC BY 4.0, via Wikimedia Commons